🧬 The Silent Revolution Inside You: Understanding Digestive Disorders from Science to Solution
📖 Prologue: The Journey Begins
Imagine this: Sarah, a 32-year-old marketing executive, sits across from me in my clinic. Her eyes tell a story of frustration. "Doctor, I feel like my body has betrayed me," she whispers. "After every meal, it's a battle—burning in my chest, cramping in my abdomen, unpredictable bathroom emergencies. I've missed meetings, skipped social gatherings, and lost confidence in my own body."
Sarah's story isn't unique. It's the story of millions worldwide who wage daily battles with their digestive systems. But here's what gives me hope: understanding is the first step to healing.
Today, we're embarking on a scientific journey through the complex world of digestive disorders—one that will empower both medical students and patients with knowledge grounded in the latest research.
📚 Chapter 1: What Are Digestive Disorders? A Scientific Definition
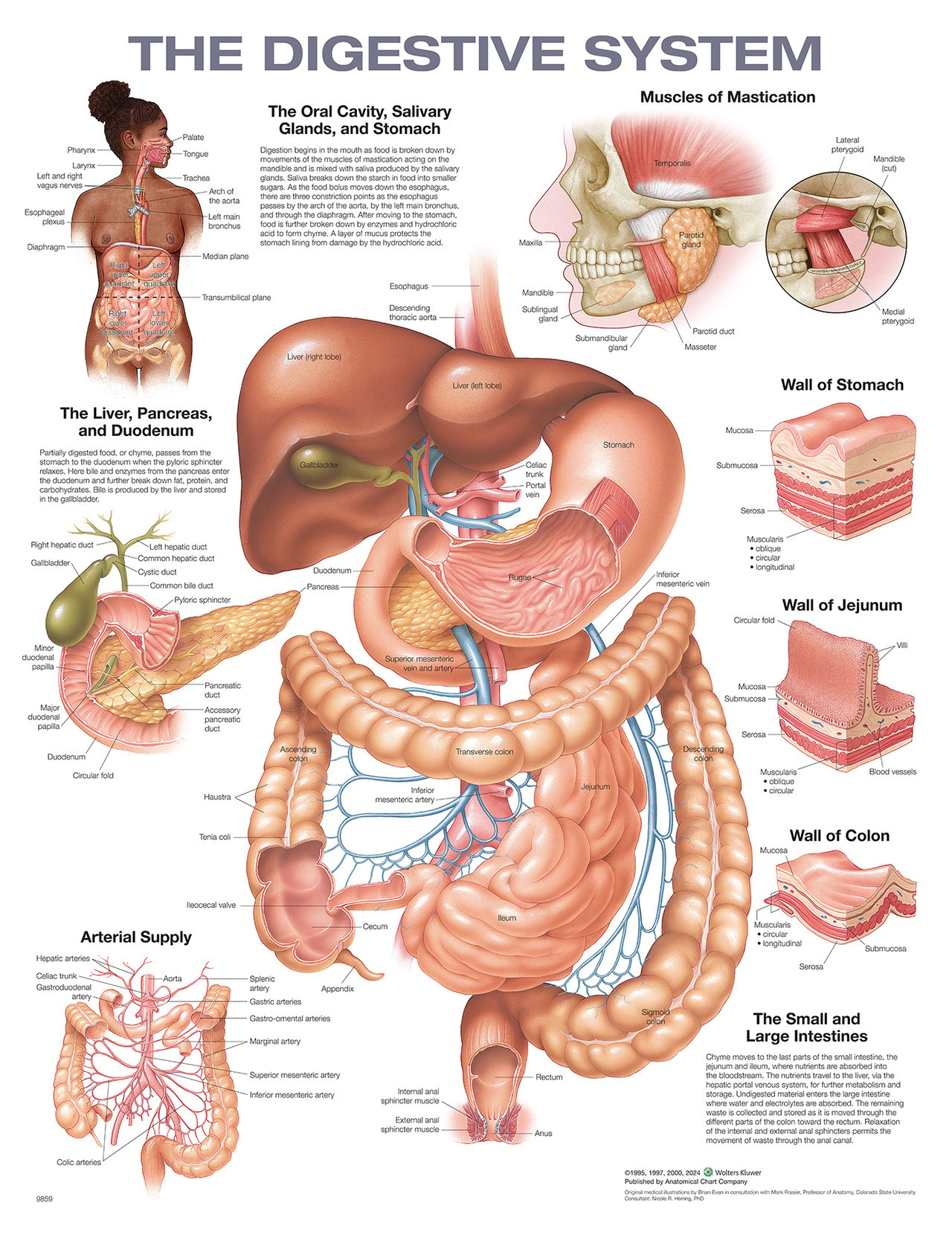
Digestive disorders encompass a broad spectrum of conditions affecting the gastrointestinal (GI) tract—from the mouth to the anus—including accessory organs like the liver, pancreas, and gallbladder. These conditions disrupt the normal processes of digestion, absorption, and elimination.
🔬 The Science Behind Digestion:
Your digestive system is a 30-foot-long muscular tube equipped with specialized organs that work in harmony to:
- Break down food into nutrients
- Absorb these nutrients into the bloodstream
- Eliminate waste products
When this delicate symphony falls out of tune, digestive disorders emerge.
🏥 Chapter 2: The Usual Suspects—Common Digestive Disorders Decoded
2.1 GASTROESOPHAGEAL REFLUX DISEASE (GERD)
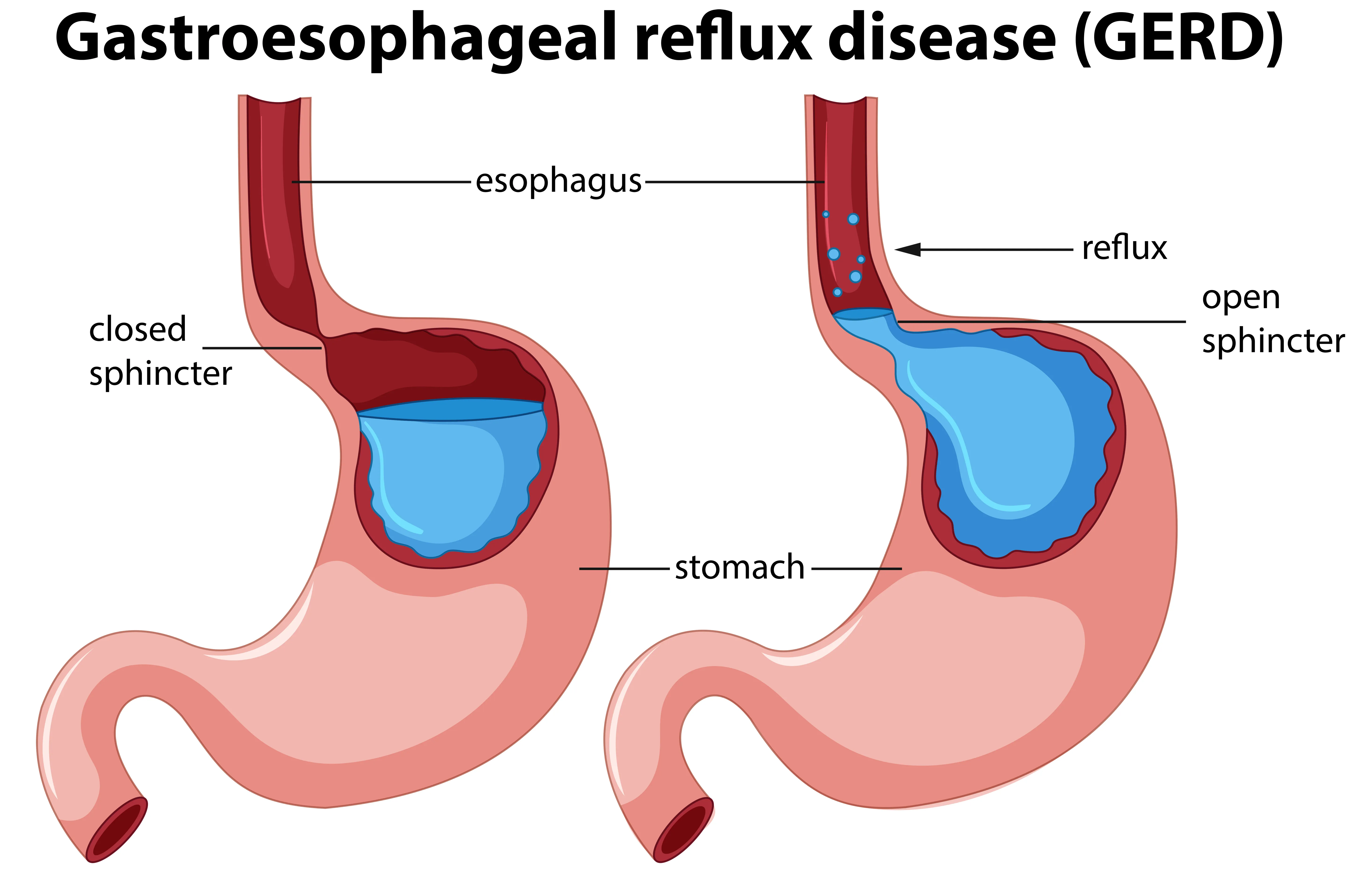
Meet Ahmed: A 45-year-old teacher who describes his symptoms as "a fire climbing up my chest every night." He's tried antacids, changed his diet, and elevated his bed, but the burning persists.
🔬 Scientific Definition
GERD is objectively defined by the presence of characteristic mucosal injury seen at endoscopy and/or abnormal esophageal acid exposure demonstrated on reflux monitoring [Katz et al., Am J Gastroenterol 2022]. The pathophysiology involves an imbalance between aggressive factors (frequency and characteristics of reflux) and defensive factors.
⚠️ Causes & Risk Factors
- Lower Esophageal Sphincter (LES) dysfunction: The valve between esophagus and stomach fails to close properly
- Hiatal hernia: Part of the stomach pushes through the diaphragm
- Delayed gastric emptying
- Obesity and increased intra-abdominal pressure
- Dietary triggers: Fatty foods, caffeine, chocolate, alcohol
🎯 Signs & Symptoms
- Classic symptoms: Heartburn (pyrosis), acid regurgitation
- Atypical symptoms: Chronic cough, laryngitis, asthma, dental erosion
- Alarm features: Dysphagia, odynophagia, weight loss, GI bleeding
🔍 Investigations
According to the 2022 ACG Clinical Guidelines:
- Empirical PPI trial: 4-8 weeks for typical symptoms without alarm features
- Upper endoscopy (EGD): For alarm symptoms or refractory cases
- 24-hour pH monitoring: Gold standard for acid exposure assessment
- Esophageal manometry: Evaluates motility disorders
💊 Treatment & Management
Lifestyle Modifications:
- Weight loss (5-10% body weight)
- Elevate head of bed 6-8 inches
- Avoid meals 2-3 hours before bedtime
- Eliminate trigger foods
Pharmacological Therapy:
- Proton Pump Inhibitors (PPIs): First-line therapy (omeprazole, esomeprazole, pantoprazole)
- H2-receptor antagonists: For mild symptoms
- Prokinetics: For delayed gastric emptying
📈 Prognosis
Excellent with appropriate treatment. Most patients achieve symptom control with PPIs. Long-term untreated GERD may lead to Barrett's esophagus and increased risk of esophageal adenocarcinoma.
2.2 IRRITABLE BOWEL SYNDROME (IBS)
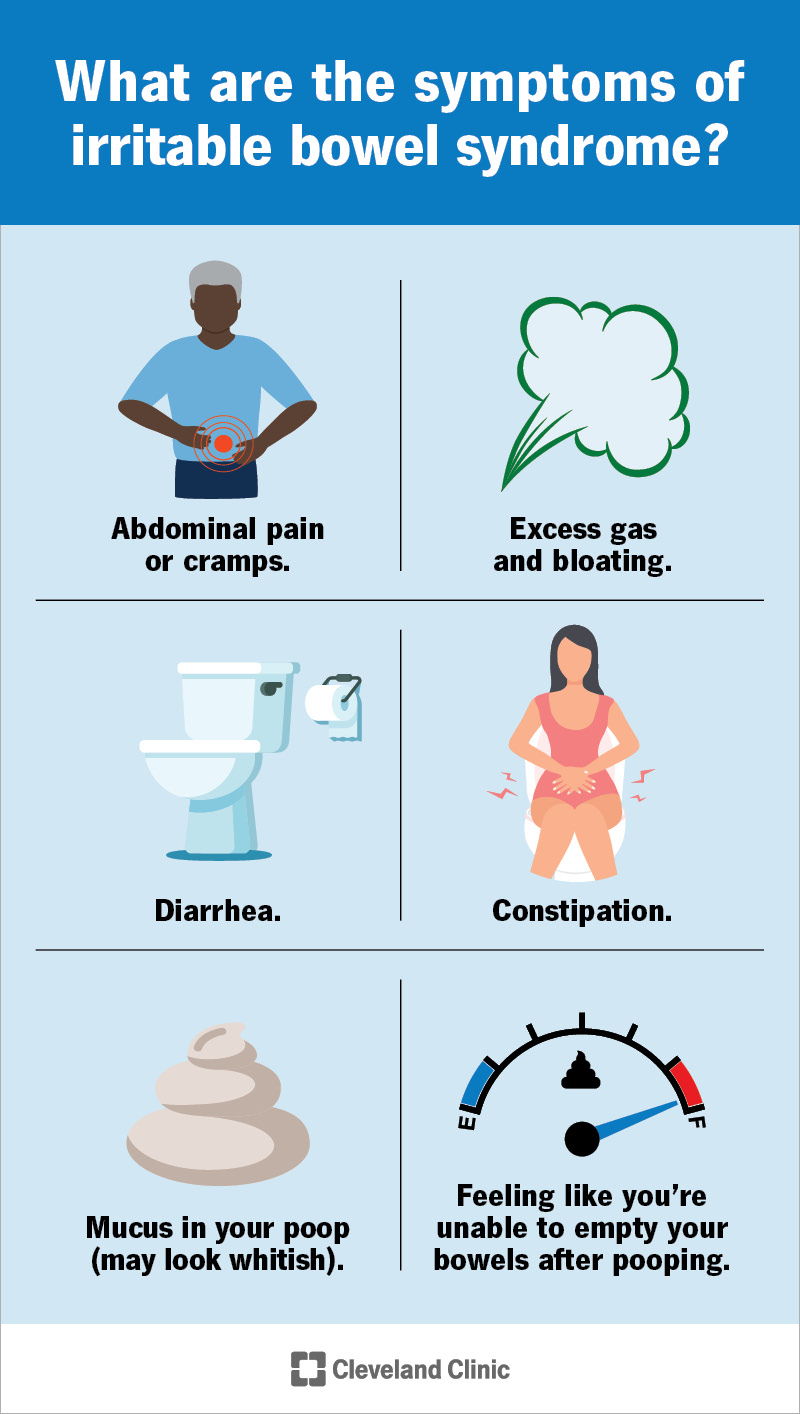
Meet Layla: A 28-year-old graphic designer who avoids long meetings and road trips. "I never know when my bowel will rebel," she confesses. "Some days it's diarrhea, other days constipation. The bloating makes me look pregnant."
🔬 Scientific Definition
IBS is a disorder of gut-brain interaction characterized by recurrent abdominal pain associated with defecation or a change in bowel frequency/form [Lacy et al., Am J Gastroenterol 2021].
Rome IV Diagnostic Criteria for IBS:
Recurrent abdominal pain, on average, at least 1 day/week in the last 3 months, associated with two or more of the following:
- Related to defecation
- Associated with a change in frequency of stool
- Associated with a change in form (appearance) of stool
⚠️ Causes & Pathophysiology
The current understanding includes [Hung & Tsai, PMC 2023]:
- Visceral hypersensitivity: Increased pain perception
- Altered gut motility: Abnormal contractions
- Microbiome dysbiosis: Imbalance in gut bacteria
- Low-grade inflammation: Post-infectious IBS
- Brain-gut axis dysfunction: Stress and psychological factors
- Food intolerances: FODMAPs, gluten sensitivity
🎯 Signs & Symptoms - IBS Subtypes
| Subtype | Characteristics |
|---|---|
| IBS-D | Diarrhea-predominant |
| IBS-C | Constipation-predominant |
| IBS-M | Mixed diarrhea and constipation |
| IBS-U | Unclassified |
🔍 Investigations
Diagnosis is primarily clinical using Rome IV criteria [Rome Foundation]:
- Limited testing recommended if no alarm features
- Basic workup: CBC, CRP/ESR, celiac serology, stool studies
- Colonoscopy: If alarm features (age >50, weight loss, rectal bleeding, family history of IBD/colon cancer)
🚨 Red Flags requiring further investigation:
- Onset after age 50
- Unintentional weight loss
- Nocturnal symptoms
- Rectal bleeding
- Family history of IBD or colorectal cancer
💊 Treatment & Management
Dietary Modifications:
- Low FODMAP diet: Reduces fermentable carbohydrates
- Fiber supplementation: Soluble fiber (psyllium)
- Regular meal patterns
- Adequate hydration
📈 Prognosis
IBS is a chronic, relapsing condition but does not increase mortality risk or progress to IBD or cancer [Lacy et al., 2021]. Quality of life can be significantly impacted, but most patients achieve satisfactory symptom control with multimodal therapy.
2.3 PEPTIC ULCER DISEASE (PUD)
Meet Karim: A 52-year-old businessman who experiences "gnawing pain" 2-3 hours after meals that wakes him at night. He finds temporary relief with food but the pain always returns.
🔬 Scientific Definition
Peptic ulcers are discontinuities in the gastric or duodenal mucosa extending through the muscularis mucosae, caused by an imbalance between aggressive factors (acid, pepsin, H. pylori, NSAIDs) and defensive factors (mucus, bicarbonate, prostaglandins, mucosal blood flow).
⚠️ Causes
Primary Causes:
- Helicobacter pylori infection (60-70% of gastric ulcers, 90% of duodenal ulcers)
- NSAID use (aspirin, ibuprofen, naproxen)
- Combination of H. pylori + NSAIDs (synergistic effect)
🎯 Signs & Symptoms
| Feature | Duodenal Ulcer | Gastric Ulcer |
|---|---|---|
| Pain timing | 2-3 hours AFTER meals | Worsened BY food |
| Pain relief | Relieved by food/antacids | No relief from food |
| Nocturnal pain | Common (1-3 AM) | Less common |
| Weight | Weight gain | Weight loss |
🔍 Investigations
Upper Endoscopy (EGD):
- Gold standard for diagnosis
- Allows biopsy for H. pylori testing
- Rules out malignancy (especially for gastric ulcers)
- All gastric ulcers should be biopsied and followed to healing
💊 Treatment & Management
H. pylori Eradication Therapy (According to 2024 ACG Guidelines [Chey et al., Am J Gastroenterol 2024]):
First-line Regimens (14 days preferred):
- Bismuth Quadruple Therapy (BQT):
- PPI twice daily
- Bismuth subsalicylate/subcitrate 4 times daily
- Tetracycline 500mg 4 times daily
- Metronidazole 500mg 3-4 times daily
- Rifabutin-based Triple Therapy:
- PPI twice daily
- Amoxicillin 1g 2-3 times daily
- Rifabutin 150mg daily
📈 Prognosis
Excellent with appropriate H. pylori eradication (90%+ cure rates). Ulcers heal in 4-12 weeks with PPI therapy. Recurrence is rare after successful H. pylori eradication (<10%).
2.4 GALLSTONE DISEASE (CHOLELITHIASIS)
Meet Fatima: A 42-year-old mother of three who experiences severe right upper quadrant pain after fatty meals that radiates to her right sh



Comments